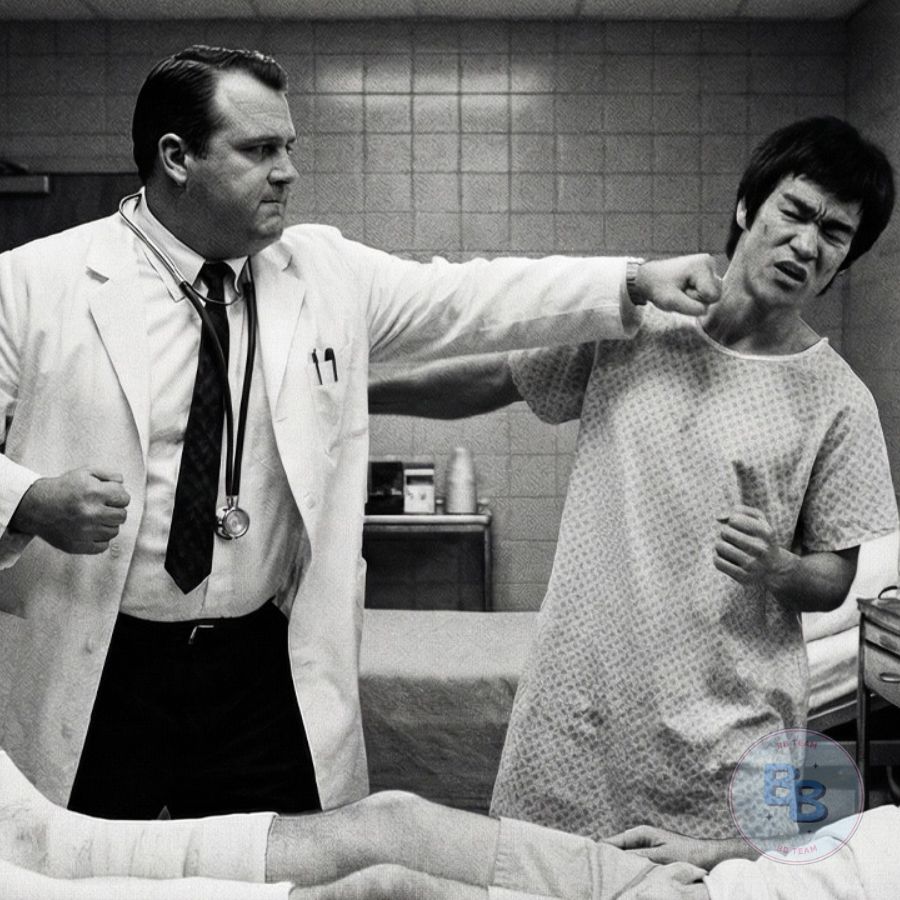
Bruce Lee was visiting his injured student in hospital when a surgeon said, “Kung fu caused this injury. Your pseudoscience cripples people. Real medicine fixes them.” March 8th, 1968, Cedars-Sinai Medical Center, Los Angeles. Dan Inosanto, Bruce’s senior student, was hospitalized with a compound femur fracture from a car accident. Dr.
Richard Morrison, chief of orthopedic surgery, 6 ft 4, 30 years of medical practice, walks in during visiting hours, sees Bruce, makes assumptions. “You’re the kung fu teacher. I’ve heard about you. Teaching people pressure points that don’t exist. Chi that can’t be measured. Mystical nonsense contradicting everything modern medicine knows. Mr.
Inosanto will heal because of surgery and science, not because of your philosophy.” Bruce responded calmly, “I’ll show you something. If you can explain it with Western medical knowledge, I’ll agree with you. But if you can’t, you acknowledge your knowledge is incomplete.” What Bruce demonstrated in the next 15 minutes forced Dr.
Morrison to question everything he thought he knew about human physiology and changed medical opinion about Eastern practices forever. 2:30 p.m., Bruce Lee walked through the automatic doors of Cedars-Sinai Medical Center carrying a small bouquet of flowers and a book. The flowers were simple daisies, nothing elaborate, because Dan Inosanto wasn’t the type of person who needed elaborate gestures.
The book was Tao Te Ching in English translation, something to help Dan pass the time, something to remind him that injury was temporary but philosophy was permanent. Bruce had been to hospitals before, didn’t like them. The smell, antiseptic, illness, suffering masked by chemicals.
The sounds, machines beeping, intercoms announcing codes, the institutional hum of fluorescent lights, the feeling sterile, controlled, places where human bodies became mechanical problems to solve rather than whole people to heal. But Dan was a student, his friend, his training partner for 4 years. If Dan was in a hospital bed, Bruce would visit, would bring flowers and books, would sit and talk, would do whatever a teacher should do when a student was hurt.
The visitors desk directed Bruce to the surgical wing. Fourth floor, west wing, room 412. Bruce took the elevator, emerged into a corridor that looked like every hospital corridor, linoleum floors, beige walls, fluorescent lighting that made everyone look slightly ill. Rooms on both sides with partially open doors revealing glimpses of patients in various stages of recovery or decline.
Bruce found room 412, knocked gently, heard Dan’s voice, strained, tired, but welcoming, say come in. The room was semi-private, two beds. Dan occupied the one by the window. The other bed was empty, sheets stripped, waiting for the next patient. Dan lay propped up slightly, his left leg suspended in a traction apparatus.
Metal frame extending from the bed, weights hanging from cables, pins inserted through bone holding everything in alignment while it healed. His left arm was in a sling. His torso was wrapped in bandages protecting broken ribs. His face was bruised, yellow and purple fading into green as the older bruises healed. He looked diminished.
This man who Bruce had seen execute perfect spinning kicks, perfect strikes, who moved with grace and power, now reduced to immobility, trapped in a mechanical contraption, dependent on nurses and doctors and medications. “Sifu,” Dan said, tried to smile, winced. Smiling hurt because breathing hurt because his ribs were broken.
“You didn’t have to come. I know you’re busy, teaching, training. You’ve got students who need you more than I do right now.” Bruce set the flowers on the bedside table, pulled up a chair, sat so he was at Dan’s eye level, not towering over him, not emphasizing Dan’s vulnerability. “You’re my student, my friend. Of course I came.
How are you feeling? Real answer, not the polite answer.” Dan exhaled slowly, carefully. Breathing was navigation through pain. “Honestly, like I got hit by a car, which is accurate because I did get hit by a car. Everything hurts. The leg hurts from the surgery and the pins and the traction.
The ribs hurt every time I breathe. The shoulder hurts every time I move. The medications make me foggy but don’t actually stop the pain, just make me care about it less. I am bored. I am frustrated. I can’t train, can’t move, can’t do anything except lie here and heal slowly. It’s driving me crazy.” Bruce understood.
Dan was a martial artist, a practitioner, someone who expressed himself through movement, through training, through physical excellence. Being trapped in a hospital bed, unable to move, unable to practice, unable to do the things that defined him, that was its own kind of suffering beyond the physical pain. “Tell me about the accident. You said drunk driver.
” Dan nodded. “Two nights ago, I was driving home from teaching a class, late, maybe 10:00 p.m. Going through an intersection, I had a green light and this guy ran a red, didn’t even slow down, just blasted through and T-boned me, spun my car into a lamp post. I remember the impact, remember the pain, remember knowing something was badly wrong with my leg.
Then EMTs, then surgery, then waking up here. They told me the other driver was drunk, 0.15 blood alcohol, nearly twice the legal limit. He walked away with a concussion and some bruises. I get this.” Dan gestured at the traction apparatus, at the hospital room, at his broken body. “How long until you’re mobile?” “Doctor say 6 to 8 weeks in traction, then they’ll remove it, put me in a cast, see if the bone align correctly, then physical therapy, maybe another 6 weeks, then gradual return to normal activities. They’re saying 6 months
before I’m fully mobile, a year before I could train seriously again. Maybe, they’re not sure. Compound fractures are complicated. The bone didn’t just break, it shattered, came through the skin. They had to put in a metal rod, had to pin fragments, had to hope everything lines up correctly as it heals.
There’s risk I might never move the same way, risk of permanent mobility loss, risk of chronic pain. They won’t know until I’m healed.” Bruce absorbed this. A year minimum before Dan could train, possibly permanent impairment. For martial artist, this was catastrophic, not fatal, not paralysis, but catastrophic in its impact on everything Dan had built his life around.
“I’ll help,” Bruce said, “however I can. Your students, I’ll cover your classes. Your training, when you’re ready to start again, we’ll adapt, modify, find ways to work around limitations. Martial arts isn’t just full mobility, it’s understanding, it’s principle. We’ll find a way.” “Thank you, Sifu. That means” Dan stopped mid-sentence, winced, breathed carefully, saw the “Talking hurts, breathing hurts, everything hurts.
They got me on morphine but it’s not enough, or maybe it is enough and I’m just not handling pain well. I don’t know. I feel weak, feel like I should be tougher than this.” “You broke three ribs and your femur. You’re not weak for feeling pain, you’re human. Give yourself permission to hurt. Give yourself permission to heal slowly. Don’t judge yourself for not being superhuman.
” Before Dan could respond, the door opened. No knock, no announcement, just opened. A man entered, 6 ft 4, early 50s, white coat, stethoscope around his neck, clipboard in hand. He had the bearing of authority, of someone used to being in charge, used to being right, used to being deferred to. Dr. Richard Morrison, chief of orthopedic surgery.
Bruce had seen his name on the whiteboard outside Dan’s room, listed as attending physician. Morrison walked directly to Dan’s bedside without acknowledging Bruce, started checking the chart hanging from the foot of the bed, examined the traction setup, pressed on Dan’s left leg. Clinical touch, checking for proper pin placement. Dan winced.
Morrison noted the response but didn’t apologize, didn’t acknowledge Dan’s discomfort, just made notes on his clipboard. “Mr. Inosanto,” Morrison said without looking up. His voice was professional, detached, the voice of someone delivering information about a mechanical system rather than talking to a suffering human being.
“Your latest X-rays show acceptable alignment. The surgical pins are holding. Bone fragments are maintaining position. Swelling is decreasing appropriately. You’re progressing adequately. Continue current pain management protocol. I’ll check you again tomorrow morning.” He turned to leave, then noticed Bruce for the first time, noticed the flowers Bruce had brought, noticed Bruce’s athletic build, his controlled way of sitting, something about him that suggested physical training, discipline, martial background. “You one of his
martial arts friends?” Morrison asked, not friendly, assessing, making assumptions. “I’m his instructor,” Bruce said, “Bruce Lee.” Morrison’s expression shifted, Recognition, but not positive recognition. Something else underneath. Disapproval, disdain. The look someone gives when they encounter something they consider beneath them.
Ah, the kung fu teacher. I’ve heard about you. You run a school in Chinatown. Teach people to jump around and make noises. Break boards. Impressive for demonstrations, I’m sure. Good party trick. The condescension was clear, deliberate. Morrison wasn’t trying to hide it. Bruce remained calm. He’d encountered this attitude before, many times.
Western professionals, doctors, academics, scientists, dismissing Eastern practices without investigating them, without understanding them, without recognizing that different approaches to human capability might both be valid. I teach martial arts, self-defense, physical conditioning, mental discipline, philosophy, practical application of principles that have been refined over thousands of years.
Philosophy, Morrison repeated, mocking, making the words sound like an insult. Is that what you call it? I call it pseudoscience, mystical nonsense dressed up as physical training. Pressure points that don’t exist anatomically, energy meridians with no basis in human physiology, chi that can’t be measured or detected by any scientific instrument, ancient wisdom that contradicts everything knows about how the human body actually works.
Mr. Inosanto is in this hospital bed because of physics, velocity, mass, impact force, kinetic energy transfer. Simple Newtonian mechanics. He’ll heal because of medicine, surgical intervention, antibiotic prophylaxis, proper immobilization, evidence-based pain management, not because of your philosophy, not because of kung fu, not because of anything Eastern medicine offers.
Science will fix him, not mysticism. Bruce felt anger flash hot in his chest, but he controlled it instantly. Let it pass through him without taking root. Getting angry would accomplish nothing. Anger would make Morrison more defensive, more certain he was right. This man needed teaching, needed his certainty challenged, needed to encounter something that would force him to question his assumptions.
But teaching required patience, required strategy, required finding the right approach. Dan tried to intervene, tried to defuse the tension building in the room. Dr. Morrison, Bruce is just visiting. He’s not interfering with treatment. We’re just talking. He brought flowers. Morrison’s expression softened slightly when he looked at Dan.
Whatever his attitude toward Eastern practices, he genuinely cared about his patients, genuinely wanted them to heal. That was clear. I’m glad you have visitors, Mr. Inosanto. Social support aids recovery. But he looked back at Bruce. I want to be clear. Your healing will happen through Western medical intervention, through the surgery I performed, through proper post-operative care, through evidence-based protocols developed over decades of research.
Please don’t let anyone fill your head with false hope about alternative treatments accelerating your recovery. Chi manipulation, acupuncture, herbal remedies. These things are placebos at best, dangerous delays of proper treatment at worst. I’ve seen patients die because they trusted traditional medicine instead of real medicine, trusted herbs instead of antibiotics, trusted acupuncture instead of surgery, ended up dead or permanently damaged because they believed ancient wisdom was equivalent to modern science. It’s not.
Science works. Tradition is superstition. Remember that. Bruce made his decision. He was going to teach this man, not through argument. Arguing never convinced anyone, just made both sides more entrenched. Through demonstration, through showing Morrison something that would force him to question, to doubt, to recognize that his framework, while extensive, while valid in its domain, was incomplete. Dr.
Morrison, Bruce said. His voice was calm, controlled, carrying authority despite being quiet. I’d like to show you something, a demonstration, right here, right now. If you can explain what I’m about to show you using only Western medical knowledge, only principles taught in Western medical schools, only mechanisms recognized by Western science, then I’ll agree with you.
I’ll publicly acknowledge that Eastern practices are pseudoscience, that traditional knowledge is superstition, that there’s nothing of value in 3,000 years of Chinese, Indian, and other Asian traditions’ understanding of human physiology. But Bruce paused, making sure Morrison was listening. If you cannot explain what I demonstrate, if what I show you contradicts or exceeds what Western medicine says is possible, if I can do things with my body that your training says shouldn’t be possible, then you acknowledge that your
knowledge is incomplete, that there might be value, real, practical, measurable value in practices you dismiss, that Eastern and Western medicine might both have pieces of truth, that integration might be superior to dismissal. Deal? Morrison stared at Bruce. Was this tiny Chinese man, 5 ft 7 at most, couldn’t weigh more than 140, challenging him? Challenging a medical doctor with 30 years of training and practice? Challenging the chief of orthopedic surgery at one of Los Angeles’ premier hospitals? This should
be amusing. Fine, Morrison said, a slight smile on his face. The smile of someone humoring a fool. Show me a magic trick. Show me your chi or pressure points or whatever mystical phenomenon you’re claiming exists. I’ll explain it with actual science, with real physiology. And then maybe you’ll stop filling my patient’s head with false hope about Eastern medicine accelerating his healing.
Maybe you’ll understand that what works in a dojo doesn’t work in a hospital, that demonstrations and board breaking aren’t the same as actual medical intervention. I’ll need equipment, Bruce said, scientific instruments, objective measurement tools, blood pressure cuff, stethoscope, EKG machine if you have one that’s portable.
I want you to measure what I’m about to demonstrate. I want data, numbers, readings you can’t dismiss as illusion or trickery or perception. I want scientific evidence. Can you get those? Morrison’s smile widened. Most pseudoscience practitioners avoided measurement, avoided objective testing, made claims enough to be unfalsifiable. But this guy was asking for scientific instruments, asking to be measured? This was unexpected, interesting.
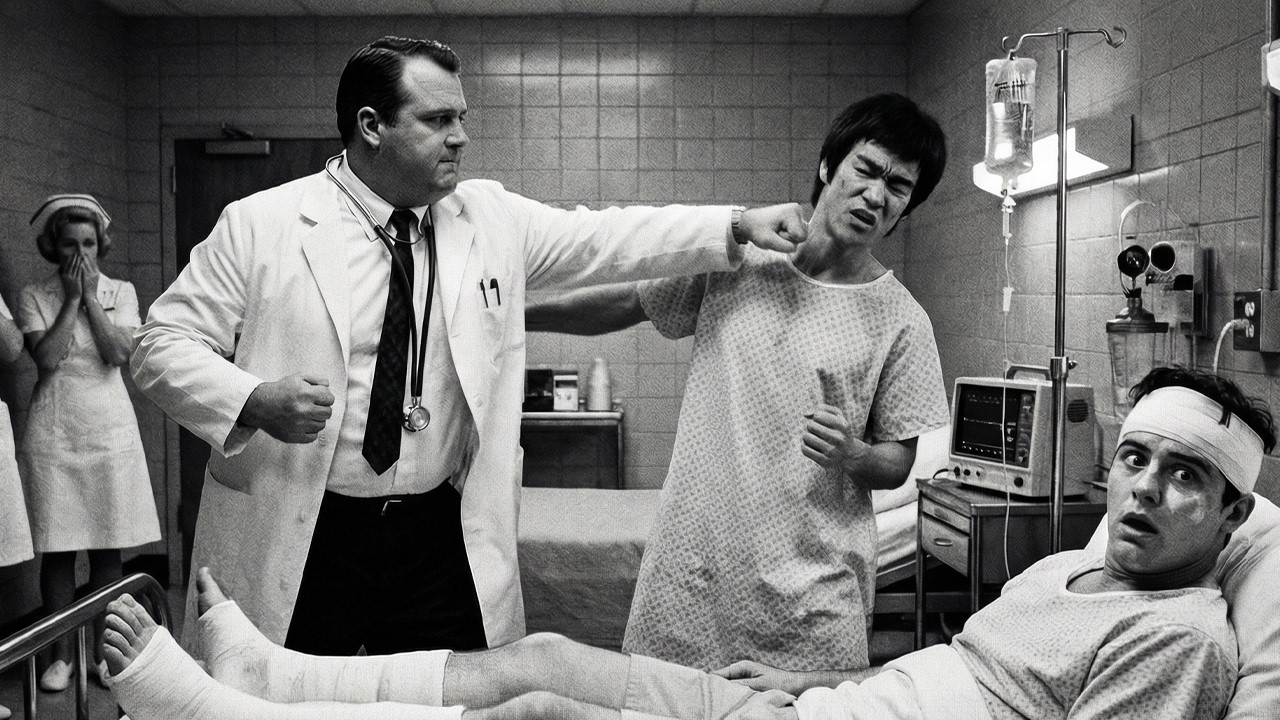
Maybe this would be more entertaining than Morrison had anticipated. Nurse Chun, Morrison called into the hallway, loud, commanding, the voice of someone used to immediate response. A moment later, a woman appeared in the doorway, 5 ft 4, late 20s, Chinese-American, navy blue scrubs, stethoscope around her neck. Nametag, Amy Chun, RN.
She’d been working this floor for 3 years. Knew Dr. Morrison well, knew his brilliance, knew his arrogance, knew his complete dismissal of anything that fell outside Western medical orthodoxy. Yes, Dr. Morrison. Bring me a blood pressure cuff, stethoscope. Actually, use mine. He handed her his stethoscope and the portable EKG from the nurses’ station.
We’re going to conduct an experiment. Going to scientifically measure some kung fu magic. The sarcasm was thick. Amy’s eyes moved to Bruce. Recognition flickered across her face. She knew who he was, not personally, but her grandmother, traditional Chinese medicine practitioner, herbalist in Chinatown, had mentioned him, had said Bruce Lee understood the old ways, understood body control, understood things that Western-trained doctors dismissed because they couldn’t measure them with their instruments.
Amy wondered what Bruce was planning, what he was about to show Dr. Morrison. She’d worked with Morrison long enough to know he was brilliant but rigid, believed Western medicine had a monopoly on truth, dismissed traditional Chinese medicine as superstition despite Amy’s grandmother’s practice helping people for 40 years.
Amy had tried once to mention acupuncture’s potential value. Morrison had shut her down with a lecture about placebo effects and confirmation bias. Maybe Bruce could crack that certainty. Maybe Bruce could show Morrison what Amy’s grandmother had been trying to tell people for decades. The body was more capable, more controllable, more extraordinary than Western medicine fully understood.
Amy left, returned 2 minutes later with equipment. Blood pressure cuff, portable EKG machine, older model, wheeled cart, requires chest leads. She set everything on the small table near Dan’s bed. By this time, another person had entered the room. Dr. Sarah Klein, first-year orthopedic resident, Morrison’s mentee, 28 years old, fresh out of medical school, bright, eager, still learning.
She’d been passing in the hallway, had heard Morrison mention an experiment, had ducked in to watch. Morrison tolerated her presence. She was his student. This would be educational for her, watching pseudoscience get debunked. Are we testing? Dr. Klein asked. This gentleman” Morrison gestured at Bruce “believes he can demonstrate physiological phenomena that Western medicine says are impossible.
He’s volunteered to be measured scientifically, objectively. We’re going to watch him fail to produce anything that can’t be explained by basic autonomic responses and placebo effect. It’ll be educational. You’ll learn how to professionally debunk alternative medicine claims. Important skill for a physician.
” Bruce stood, moved to the center of the small room. “Before we begin, establish my baseline, normal resting vitals. So, you know what’s normal for me, so you can measure changes accurately.” Morrison nodded. Professional. Whatever his personal opinions, he was a scientist, would do this correctly. “Sit, please. Arm out.” Bruce sat in the chair he’d been using, extended his right arm.
Morrison wrapped the blood pressure cuff around Bruce’s bicep, pumped it tight, watched the gauge as he released the pressure, listened with his stethoscope. “110 over 70.” Morrison announced. “Normal. Textbook normal adult blood pressure.” He moved the stethoscope to Bruce’s chest, listened, counted. “Heart rate 58 beats per minute.
Low normal, consistent with athletic conditioning. Endurance athletes often have resting heart rates in the 50s. Nothing unusual. Good cardiovascular fitness, but not extraordinary.” Morrison made notes on his clipboard, establishing baseline, being thorough. “Respiratory rate.” Bruce asked. Morrison counted Bruce’s breaths for 30 seconds, multiplied by two. “14 breaths per minute.
Normal adult resting respiratory rate is 12 to 20. You’re mid-range. Again, nothing unusual.” “Good.” Bruce said. “Now watch. Time how long this takes. Measure continuously if you can. I want you to see this is voluntary, controlled, not accident, not medical condition, deliberate demonstration of trained capability.
” Bruce closed his eyes, settled into the chair, let his body relax completely, began breathing slowly, deliberately, a technique he’d learned years ago, Qigong method taught by masters in Hong Kong, breathing that connected mind and body, breathing that gave access to functions Western medicine said were autonomic, automatic, uncontrollable, purely biological.
The room went quiet, everyone watching. Morrison skeptical, but curious. Dr. Klein interested. Amy hopeful. Dan watching his teacher, wondering what Bruce was about to demonstrate. Morrison waited 1 minute, then took blood pressure again. “95 over 60. Dropped 15 points systolic, 10 points diastolic. Consistent with relaxation response.
Activates parasympathetic nervous system. Well-documented Western physiological phenomenon. Nothing mystical. Meditation, controlled breathing, progressive relaxation all produce this effect. We teach this to patients for stress management.” Bruce didn’t respond, didn’t open his eyes, just continued breathing.
“Slow now, deeper, more controlled.” Morrison checked heart rate. “52 beats per minute. Down six beats. Again, consistent with relaxation response. Vagal activation reduces heart rate. Basic parasympathetic function.” Another minute passed. Morrison measured again. “46 beats per minute.” His tone shifted slightly, still confident, but less dismissive. 46 was getting low.
Still within normal range for elite athletes, but Bruce hadn’t been exercising, hadn’t been preparing his body through physical exertion, which is sitting and breathing. “One more minute.” Morrison measured. “41 beats per minute.” Now Morrison frowned. 41 was approaching bradycardia territory, dangerously low heart rate, the kind that required medical attention in most patients.
“You’re doing something with your breathing, bearing down, stimulating vagal response through mechanical pressure. Put your hand on my chest.” Bruce said quietly, eyes still closed, voice calm. “Feel my breathing. Verify I’m not holding my breath, not bearing down, not doing any mechanical vagal stimulation, just breathing.” Morrison hesitated.
This felt like a trick, but he was a scientist. Verification was important. He placed his hand on Bruce’s chest, felt the slow, steady rise and fall, continuous breathing, no holding, no straining, no mechanical pressure, just slow, controlled respiration. But the heart rate continued dropping. Two minutes later, Morrison measuring every 30 seconds now, fascinated despite himself.
The reading was 35 beats per minute. “This is bradycardia.” Morrison said, his voice uncertain now, the confidence wavering. “This is dangerously low. Heart rates this low usually require intervention. Pacemaker, atropine. This shouldn’t be possible through voluntary control. The autonomic nervous system isn’t under conscious control.
That’s why it’s called autonomic. We can influence it indirectly through breathing, through relaxation, but we can’t directly control it. Can’t voluntarily slow our heart rate to this degree. It’s not physiologically possible.” “In the West” Bruce said, eyes still closed, voice still calm “it’s not possible because you don’t train it.
Don’t believe it’s possible, so you never try, never develop the technique. But in the East, China, India, Tibet, Japan, we’ve been training voluntary control of autonomic functions for 3,000 years. Different traditions, different names. Qigong, Tummo, Pranayama, Neigong. Different techniques, but same principle. The body is more controllable than you believe.
The autonomic nervous system can be trained, can be influenced, can be directed through breathing, through focus, through techniques passed down for millennia. This” Bruce gestured at Morrison’s stethoscope, at the heart rate of 35 beats per minute that shouldn’t be possible “this is basic level, entry-level skill.
What master practitioners can do goes far beyond this.” Morrison’s face showed confusion, doubt, the first cracks in his certainty. He was watching something that contradicted his training, contradicted what he’d been taught was possible. The autonomic nervous system was autonomic, automatic, beyond conscious control. That was fundamental.
That was taught in first-year medical school. That was established scientific fact. But Bruce was sitting here voluntarily lowering his heart rate to levels that should require medical intervention, and doing it just through breathing, through focus, through something Morrison had dismissed as mysticism. Dr. Klein spoke up.
Her voice carried wonder. “Dr. Morrison, this is I don’t understand. Autonomic nervous system isn’t under voluntary control. We learn that. It’s in every textbook. How is he doing this?” Morrison didn’t answer, couldn’t answer, didn’t have an answer. Everything in his training said this wasn’t possible. But his stethoscope, his scientific instrument, his objective measurement tool, was telling him it was happening.
Three minutes after Bruce started, the heart rate was 30 beats per minute. The blood pressure was 80 over 50. Both readings were in dangerous territory for most patients. But Bruce showed no distress, no dizziness, no confusion, just calm, controlled breathing, deliberate demonstration of capability that shouldn’t exist. “Enough.
” Morrison said, not commanding, almost pleading. “Stop. This is dangerous. Heart rate this low.” Bruce opened his eyes, smiled slightly, not mocking, just acknowledging. “It’s not dangerous when you’re trained, when you know how to control it. Watch.” Bruce shifted his breathing, changed the pattern. Faster now, shorter breaths, different technique.
Morrison watched, stethoscope still on Bruce’s chest, and felt the heart rate accelerate. Felt it rise as deliberately as it had fallen. 60 seconds later, Bruce’s heart rate was back to 58 beats per minute, exactly where it had started. Blood pressure was back to 110 over 70. Everything returned to baseline, voluntarily, under complete control. Morrison stepped back.
His face showed something he rarely felt, uncertainty. “That’s one metric.” Morrison said, defensive now, scrambling to maintain his framework. “Heart rate. Could be genetic anomaly. Could be There might be explanations. I need to research. But this is one example, one function. Doesn’t prove.” “Then let me show you another.” Bruce said.
He stood, removed his shirt. His torso was lean, defined, every muscle visible, the physique of someone who’d spent decades training, refining, understanding his body at a level Morrison had never considered possible. “What are you going to show me now?” Morrison asked, still skeptical, but shaken, still defensive, but curious. “Muscle control. Isolation.
Western medicine says muscles contract in groups, functional groups, motor units. You can’t contract one muscle without its synergists and stabilizers. Voluntary muscle control is imprecise. Groups, not individual muscles. Correct. Generally correct. Motor control is organized by function, not by individual muscle.
When you flex your bicep, you’re activating multiple muscles. Biceps brachii, brachialis, brachioradialis, along with stabilizers in the shoulder and forearm. You can’t voluntarily activate just one. Can’t you? Bruce asked and demonstrated. His left pectoral muscle contracted visibly, distinctly. Just the left. While his right pectoral remained completely relaxed.
Then his right contracted, left relaxed. He alternated. Left, right, left, right, making his pectoral muscles dance independently. Morrison stared. That’s That’s just the pectoralis major. Large muscle, easier to isolate. Bruce’s left external oblique contracted. Just that one muscle on his left side, creating ripple in his abdomen. Then just the right external oblique.
Then the upper rectus abdominis. Then the lower rectus. Each muscle contracting individually, independently, precisely. Creating patterns. Creating wave-like motion through his core musculature that looked impossible because it was impossible according to Western understanding of motor control. Dr. Klein gasped.
How How are you doing that? Training, Bruce said simply. Awareness. Thousands of hours of training to understand my body. To map every muscle. To develop voluntary control of individual fibers. Not groups. Individual muscles. Western medicine says it’s impossible because Western medicine doesn’t train it. Doesn’t believe it’s possible.
But in Chinese martial arts, in Qigong, in Neigong, in advanced practice, this is standard. This is what mastery looks like. Complete body awareness. Complete control. Amy Chen watched with growing excitement. This was what her grandmother had tried to explain. What traditional Chinese medicine practitioners understood but couldn’t always articulate to Western doctors.
The body was more controllable, more trainable, more extraordinary than Western medicine acknowledged. Bruce was demonstrating it. proving it. Making it undeniable. Morrison’s certainty was crumbling. But he wasn’t ready to surrender completely. Wasn’t ready to admit he might be wrong. Muscle control. Fine. Impressive party trick.
But that doesn’t mean chi exists. Doesn’t mean meridians are real. Doesn’t mean I’m not claiming chi is a mystical energy, Bruce interrupted. I’m not claiming meridians are magical pathways. I’m claiming that traditional Chinese medicine developed a framework, a model for understanding body control that works. That produces results.
Whether the framework is literally true or metaphorically true doesn’t matter if the techniques work. Western medicine has its model. Nervous system, motor units, autonomic functions. Chinese medicine has its model. Chi, meridians, pressure points. Both are maps. Neither is the territory. But both maps lead to real destinations.
Both produce real results. Your map says voluntary heart rate control is impossible. My map says it’s trainable. We just watched me do it. Which map is more accurate? Morrison had no response. Was watching his certainty dissolve. Was feeling his framework, the framework he’d built his entire career on. The framework he taught to hundreds of residents and medical students, crack under the pressure of direct demonstration.
Let me show you one more thing, Bruce said. Then we’ll talk. Then I’ll explain. Then maybe you’ll understand why dismissing Eastern practices as pseudoscience is arrogant and limiting. What else could you possibly show me? Morrison asked. His voice was quiet now. Defensive but genuinely curious. Temperature control.
Western medicine says body temperature is regulated automatically. Homeostasis. Hypothalamus controls thermoregulation. You can’t voluntarily raise or lower your body temperature in specific locations. Your entire body warms or cools together. Systemic regulation. Yes. Yes. Thermoregulation is autonomic. Whole body function.
You can’t just make your left hand warmer than your right hand. That’s not how physiology works. Put your hand on my left palm, Bruce said. Extended his left hand. Morrison hesitated. Then placed his hand on Bruce’s left palm. Felt normal temperature. Maybe slightly cool. Room temperature circulation. Now my right palm. Bruce extended his right hand.
Morrison moved his hand. Felt the same. Normal temperature. Now watch. Wait 30 seconds. Then touch again. Bruce closed his eyes. Breathed. Focused. Amy recognized the technique. Her grandmother had mentioned it. Tummo. Tibetan Buddhist practice. Generating heat through controlled breathing and visualization.
Monks in Tibet had been studied doing this. Generating enough heat to dry wet sheets draped over their bodies in freezing temperatures. Scientific studies had measured it. Temperature differentials of 10, 15° C in controlled conditions. 30 seconds later, Bruce opened his eyes. Try again. Morrison placed his hand on Bruce’s left palm. Cool. Same as before.
Then his right palm. Heat. Significant heat. Like touching a warm stove. Not burning. But notably, measurably warmer than Bruce’s left hand. Then Morrison’s own hand. Then room temperature. What how? Morrison pulled his hand back. Stared at Bruce. At this man who was systematically destroying everything Morrison thought he knew about human physiology.
I focused blood flow to my right hand. Dilated the blood vessels voluntarily. Increased circulation. Generated heat through metabolic activity that I controlled. Your framework says this is impossible. My framework, the Eastern framework, says this is trainable. We just demonstrated it. Three times now. Heart rate control. Muscle isolation. Temperature control.
Three autonomic functions that Western medicine says cannot be voluntarily controlled. I just controlled all three. Voluntarily. Deliberately. Through techniques developed over 3,000 years in Eastern traditions. So tell me, Dr. Morrison, is your knowledge complete? Or is it possible, just possible, that Eastern practices contain real value that Western medicine hasn’t integrated yet? Morrison sat down heavily in the chair Bruce had vacated.
His face showed a man whose worldview was collapsing. Whose certainty was shattered. Whose foundation was cracking. Dr. Klein looked at Morrison. Her mentor. Her teacher. The man who’d spent months teaching her to dismiss alternative medicine as pseudoscience. And she saw doubt. She saw confusion. She saw someone forced to confront evidence that contradicted his beliefs. Dr.
Morrison, Dr. Klein said quietly. I don’t understand what we just saw. But we saw it. We measured it. We verified it. He lowered his heart rate to 30 beats per minute voluntarily. He contracted individual muscles independently. He created temperature differential in his own hands. These things shouldn’t be possible. But they happened.
We witnessed them. What does that mean? Morrison didn’t answer immediately. Sat in silence. Processing. Rethinking. Questioning. Finally, he looked at Bruce. Teach me, Morrison said. His voice was different now. Humble. Genuine. The voice of a student asking a teacher for knowledge. Explain this. Help me understand.
Show me how this is possible. Not just that it’s possible. We’ve established that. Show me how. What’s the mechanism? What’s the technique? How does someone train this? How do I integrate this understanding with what I know? Help me understand. Bruce smiled. Not a triumphant smile. A teaching smile. He broken through Morrison’s defenses.
Had created an opening for learning. Had transformed a skeptic into a student. Now the real teaching could begin. First, Bruce said, we need to establish something. I’m not asking you to abandon Western medicine. Western medicine is extraordinary. Life-saving. Based on rigorous scientific method. It’s produced miracles. I respect it deeply.
What I’m asking is that you recognize Western medicine is incomplete. Not wrong. Incomplete. It knows how the body works. Anatomy, physiology, biochemistry. Eastern medicine knows how to make the body work differently. How to control what you say is uncontrollable. How to access capabilities you say don’t exist. Both are true. Both are valuable.
Integration is superior to dismissal. Can you accept that? Morrison nodded slowly. I can accept that. Today proved my knowledge is incomplete. Proved there are capabilities I didn’t know existed. Proved 3,000 years of Eastern practice must contain real insights even if I don’t understand the mechanisms yet.
I can accept that. What I need now is understanding. Framework. How does someone voluntarily control heart rate? What’s actually happening physiologically? How can I explain this to my residents? How can I integrate this into my practice? Then let’s talk, Bruce said. Let’s bridge the gap between East and West.
Let’s build a framework that incorporates both. Let’s start with what you just saw and work backward to mechanism. Let’s find where your knowledge and my knowledge overlap, where they complement each other, where integration creates something neither tradition has alone. And they talked for 2 hours. Bruce explaining technique, Morrison asking questions, Dr.
Klein taking notes, Amy Chan contributing perspective from her grandmother’s traditional Chinese medicine practice, Dan Inosanto watching his teacher transform a hostile critic into an eager student. Bruce explained vagal tone, how breathing techniques could stimulate the vagus nerve, how sustained practice could increase vagal activation, how Eastern breathing practices were essentially training the parasympathetic nervous system to respond to voluntary cues.
Explained proprioception, how Chinese martial arts developed extraordinary body awareness through forms, through stance training, through techniques that require precise control, how that awareness could extend to individual muscles. Explained thermogenesis, how controlled breathing, visualization, and metabolic activation could generate heat, how Tibetan monks have been studied demonstrating this, how the technique could be localized through focused attention and directed blood flow.
Morrison listened, asked questions, took notes. His scientific mind was engaging now, not dismissing but analyzing, not rejecting but integrating. He asked about mechanisms, about reproducibility, about whether these capabilities could be taught systematically or required innate talent, about whether Western medical understanding of nervous system anatomy could explain the phenomena Bruce had demonstrated.
Bruce answered patiently, explained that these capabilities were trainable, not innate, that anyone could develop them with proper instruction and sufficient practice, that it took years, sometimes decades, but that the human body’s potential far exceeded what Western medicine typically accessed, that traditional Chinese medicine’s framework of chi and meridians was a useful model even if it didn’t correspond exactly to Western anatomical structures, that the map wasn’t a territory but a useful map could lead to real destinations. Think
of it this way, Bruce said. Western medicine maps the body using nervous system, circulatory system, muscular system. Chinese medicine maps the body using meridians, pressure points, energy flow. Different maps, different language, but both describe the same territory, the human body. Both can be used to navigate that territory effectively.
Your map is more precise about structure. Our map is more precise about function and control. Integration means using both maps, using anatomical precision to understand what’s happening, using traditional techniques to make it happen. Morrison was processing, integrating. His face showed concentration. The heart rate control you demonstrated.
From a Western perspective, you were activating the vagus nerve, stimulating parasympathetic response, but you were doing it voluntarily, precisely to a degree I’ve never seen. How? What’s the actual technique? Breathing pattern first, Bruce explained. Slow, deep abdominal breathing activates parasympathetic tone.
You know this already, but most people stop there. What Eastern practices add is awareness, conscious attention to the physiological response, feeling the heart rate slow, feeling the blood pressure drop. Most Western practitioners use breathing for relaxation, but remain unconscious of the specific effects. Eastern practice trains conscious awareness of those effects.
Once you become aware, once you can feel your heart rate changing, you could begin to voluntarily influence it more precisely. You focus attention on the sensation of heartbeat. You visualize it slowing. You use breathing as the initial trigger, but mental focus as the fine control. Over time, months, years, the voluntary control becomes more precise, more reliable, more dramatic.
So it’s biofeedback, Morrison said. Conscious awareness of autonomic functions allowing voluntary influence. Western medicine has studied this. We know biofeedback works, but I’ve never seen it developed to the degree you just demonstrated because Western biofeedback training is limited by belief about what’s possible.
You teach patients to influence heart rate slightly, five, 10 beats per minute, because that’s what you believe is achievable. But Eastern traditions, unburdened by Western limitations, have been pushing the boundaries for thousands of years, finding the actual limits rather than the assumed limits. The human body is capable of extraordinary things, but only if you believe those things are possible and train accordingly. Dr.
Klein spoke up. Could you teach this? Could you teach medical students or doctors these techniques? Could this be integrated into medical practice? For pain management, stress reduction, rehabilitation? Bruce considered. Yes, but it would require changing how medicine is taught. Currently, Western medical education treats the body as passive object, something that’s examined, diagnosed, treated from the outside.
Eastern practice treats the body as active partner, something you inhabit, control, work with from the inside. Both perspectives are valuable, but Western medicine would need to add the internal perspective, add training in body awareness, in voluntary control of autonomic functions, in accessing capabilities that currently aren’t taught because they’re assumed not to exist. Morrison was nodding.
There’s precedent. We teach anatomy by dissecting cadavers, external perspective, but we also teach doctors to be aware of their own bodies, their own stress responses, their own physical limitations. What you’re describing is extending that internal awareness more systematically, making it part of medical training rather than optional wellness practice. Exactly, Bruce said.
And it has practical applications. For patients like Dan, Bruce gestured at his injured student. Pain management is critical. Your morphine helps, but has side effects, addiction risk, cognitive impairment. What if Dan could be taught to modulate his own pain response? Not eliminate it.
Pain serves a purpose, signals injury, prevents further damage, but reduce it, control it, access his body’s natural pain management systems more effectively. Morrison looked at Dan, at his patient who’d been lying there in obvious discomfort despite medication. Can you teach him that? Can you teach pain management technique that would actually work, that I could measure objectively? I can try if Dan is willing, if you’re willing to observe and measure.
We can make it a collaborative experiment. Eastern technique applied to Western medical context, measured scientifically, documented objectively. Dan spoke for the first time in hour. His voice was strained but interested. I’m willing. I’m desperate. The morphine makes me foggy but doesn’t stop the pain.
If there’s another way, if you can teach me to manage this better, I’ll try anything. Bruce turned to Dan, moved to his bedside. The pain is worst where? The ribs. Every breath pulls on them. It’s constant. Can’t escape it. The leg hurts, too, but it’s duller. The ribs are sharp, stabbing. Makes breathing difficult, which makes everything else worse.
Okay, I’m going to teach you a breathing technique. It will seem counterintuitive, breathing to reduce pain caused by breathing, but trust me, this technique has been used for thousands of years. It works. Dr. Morrison will measure your vitals before and after. We’ll see if it has objective effect. Morrison positioned himself with a stethoscope and blood pressure cuff.
Current heart rate, 72 beats per minute. Blood pressure, 130 over 85. Elevated, consistent with pain and stress. Respiratory rate, 20 breaths per minute. Also elevated, shallow breathing to avoid rib pain. Baseline established. Bruce began teaching Dan, speaking quietly, guiding him through the technique. Close your eyes.
Focus on your breathing. Don’t try to breathe deeply, that hurts. Just breathe normally. Feel the breath. Don’t judge it. Don’t fight it. Just observe. Where does it hurt most? When you inhale or exhale? Inhale, expanding the ribs. That’s when it stabs. Good. Now here’s what we’ll do. We’ll extend the exhale. Make it longer than the inhale.
Not deeper, longer. Take a normal inhale, however much doesn’t hurt too badly, then exhale slowly, very slowly. Count to five as you exhale. Don’t force it. Just extend it gently. Try it. Dan tried, inhaled carefully, exhaled slowly, counted to five, looked surprised. That That didn’t hurt as much.
Why? Because you’re activating your parasympathetic nervous system. Extended exhale stimulates vagal response, reduces pain perception, Reduces muscle tension. The intercostal muscles between your ribs, they’re tensing in anticipation of pain. That tension makes the pain worse. The extended exhale helps them relax. Breaks the cycle. Keep doing it.
Five count exhale. Natural inhale. Find a rhythm. Let your body settle into it. Dan continued, “Breathing slowly.” Morrison watched the monitors. Watched the readings change. After 5 minutes, heart rate 68, down four beats. Blood pressure 125 over 80. Starting to drop. Respiratory rate 18. Slower. He’s breathing more deeply despite the rib injury. After 10 minutes, heart rate 62.
Blood pressure 115 over 75. Respiratory rate 16. He’s relaxing measurably. Bruce continued guiding Dan. “Now add visualization. As you exhale, visualize the pain. See it as color, whatever color feels right. Red, black, whatever you associate with pain. As you exhale, visualize that color leaving your body, flowing out with your breath.
Don’t force it. Don’t try too hard. Just gently visualize pain leaving with each exhale. Cool, soothing breath coming in. Warm, pain-carrying breath going out.” Dan’s face started to relax. The tension lines around his eyes softened. His jaw unclenched. His shoulders dropped slightly despite the sling. After 15 minutes, heart rate 58.
Blood pressure 105 over 70. Respiratory rate 14. These are normal resting vitals. Better than normal for someone with his injuries. The pain should be preventing this level of relaxation. Bruce asked Dan quietly, “How’s the pain now? Scale of 1 to 10. Where is it?” Dan answered without opening his eyes. “Was an eight. Constant eight. Now it’s maybe a five.
Still there. Still hurts, but duller. More distant. Like I’m aware of it, but it’s not consuming me. I can breathe without that stabbing sensation. This is the best I’ve felt since the accident.” Morrison stared. He’d given Dan morphine. Professional-grade pain medication. It had reduced Dan’s pain from 10 to eight. Two points.
Bruce had taught Dan a breathing technique. Just breathing and visualization and reduced it from eight to five. Three points. Better than the morphine. Without side effects. Without addiction risk. Without cognitive impairment. “This is extraordinary,” Morrison said. His voice carried wonder now, not skepticism. “This is measurable pain reduction without pharmaceutical intervention.
This is If this can be replicated, if this can be taught systematically, if this works for other patients, this could change pain management protocols. This could reduce opioid dependence. This could give patients agency over their own pain instead of making them passive recipients of medication.” Bruce nodded. “This is basic level.
Entry-level technique. Advanced practitioners can do more. Can influence healing rate. Can reduce inflammation. Can access pain management so effective they can undergo surgery without anesthesia. This has been documented. Chinese patients undergoing major surgery with only acupuncture for pain control, filmed, measured, verified.
I’m not saying eliminate western pain medication. I’m saying supplement it. Give patients tools. Teach them what their bodies can do. Empower them.” Amy Chin had been watching everything. Her eyes were shining. “This is what my grandmother does. What traditional Chinese medicine practitioners have been doing for thousands of years.
But western doctors dismiss it because it doesn’t fit the model. Don’t measure it. Don’t study it. Just reject it. What you just demonstrated, that should be taught in nursing school. In medical school. Every patient should learn basic pain management technique. Every healthcare provider should understand this is real.
This is effective. This is valuable.” Morrison looked at Amy. Really looked at her for the first time. Saw past the nurse to the person. To someone who’d been trying to tell him about traditional Chinese medicine for years. Someone he dismissed. “Your grandmother practices traditional Chinese medicine? For 40 years. In Chinatown. Herbalist.
Acupuncturist. She’s helped thousands of people. People western doctors couldn’t help or wouldn’t help. I grew up watching her work. Watching patients come in suffering and leave relieved. Western doctors told me it was placebo. Told me it wasn’t real. But I saw it. I knew it was real.
I just couldn’t prove it in language western doctors would accept.” “I’d like to meet her,” Morrison said. “I’d like to learn. I’ll spend 30 years dismissing practices I didn’t understand. Today showed me that dismissal was arrogant. Limiting. There’s real value here. Real capability. I want to understand it. Want to integrate it.
Want to become a better doctor by learning what the East knows that the West hasn’t discovered yet.” Bruce smiled. “That’s exactly the right attitude. Not abandoning your training. Not replacing western medicine with eastern medicine. Integrating. Learning. Expanding. The human body is more extraordinary than either tradition fully comprehends.
But together, western science and eastern practice, together we might get closer to complete understanding.” Dr. Klein was furiously taking notes. “I want to learn this, too. Want to study with you. Want to understand how to teach patients these techniques. This is This is what medicine should be. Not just treating disease, but empowering health.
Not just fixing broken bodies, but teaching people to access their bodies’ inherent capabilities.” Morrison stood. Extended his hand to Bruce. “I apologize for my arrogance. For my dismissal. For assuming western medicine had a monopoly on truth. You’ve shown me I was wrong. Shown me that being a good doctor requires humility.
Requires openness to learning. Requires recognizing that 3,000 years of eastern tradition might contain insights western science hasn’t discovered yet. Thank you for teaching me. For being patient with my skepticism. For demonstrating rather than arguing. You’re a good teacher. I’d be honored to become your student. In this arena, at least.
” Bruce shook Morrison’s hand. “You’re a good doctor. A good scientist. Good scientists change their minds when presented with evidence. You just did. That’s not weakness. That’s integrity. That’s what makes science work. Not defending old paradigms, but building better ones when the old ones prove incomplete. I’d be honored to work with you.
To help bridge western and eastern medicine. To teach what I know while learning what you know. Together, we might actually help people more effectively than either tradition alone.” They talked for another hour. Planning. Discussing. Morrison wanted to study with Bruce. Wanted to learn these techniques himself before trying to teach them to others.
Wanted to bring rigorous scientific measurement to eastern practices. Wanted to document what worked, what didn’t, what could be explained by western mechanisms, and what might require expanding western understanding. Bruce agreed. Offered to teach Morrison. Offered to demonstrate techniques at the hospital.
Offered to work with patients under Morrison’s supervision. Teaching pain management. Teaching breathing. Teaching body awareness and voluntary control. All documented. All measured. All scientifically rigorous. Dr. Klein wanted to participate. Amy Chin volunteered to help coordinate. To introduce Morrison to her grandmother. To serve as bridge between the communities.
Dan lay in his hospital bed. Still practicing the breathing technique Bruce had taught him. Still experiencing pain relief better than morphine had provided. Grateful that his injury had catalyzed this meeting between his teacher and his doctor. At 5:00 p.m., Bruce prepared to leave. He’d been at the hospital for two and a half hours.
Had come to visit an injured student. Was leaving having transformed a skeptical surgeon into an eager student of eastern practices. “I’ll come back tomorrow,” Bruce told Dan. “Keep practicing the breathing. It’ll get easier. More effective. Your body is learning. Give it time.” “Thank you, Sifu. For visiting. For teaching the pain technique.
For” Dan gestured at Morrison. “For teaching him. That was something special. Watching you demonstrate voluntary control. Watching his certainty crack. Watching him become humble. That was masterful teaching.” Bruce nodded. He was ready. Sometimes the most defensive students become the most dedicated once their defenses break. Morrison is a real scientist.
Real scientists follow evidence even when it contradicts their beliefs. He’ll learn quickly. And his learning will help many people.” Morrison walked Bruce to the elevator. “When can we start? When can I begin training? I have a sabbatical coming up in two months. I could dedicate serious time. Could come to your school. Could practice daily.
Come whenever you’re ready.” “I teach Tuesday and Thursday evenings. 7:00 to 9:00. You can observe. Participate. Learn the basics. The advanced material, the body control demonstrations I showed you today, that takes years. But the fundamentals that are useful for medical practice, breathing, awareness, basic voluntary control of heart rate and pain response, those could be learned in months, practiced systematically, taught to others.
I’ll be there Thursday this week. I’m not waiting 2 months. I’m starting now. This is too important.” They shook hands again. Bruce stepped into the elevator. The doors closed. Morrison stood in the hallway, alone, processing everything that had happened. 2 hours ago he’d been certain, certain Western medicine was superior, certain Eastern practices were pseudoscience, certain his knowledge was complete.
Now he was uncertain, uncertain about everything he’d been taught, uncertain about the limits of human capability, uncertain about the boundaries between science and mysticism, between evidence and tradition, between what was known and what was possible. But that uncertainty felt good, felt like growth, felt like the beginning of real learning. Dr.
Klein found him in the hallway. “Dr. Morrison, are you okay?” Morrison smiled. “I’m better than okay. I am humble. I am uncertain. I’m aware of how much I don’t know. That’s the best possible state for learning. I’ve spent 30 years being certain, being arrogant, being dismissive of practices I didn’t understand. Today that ended.
Today I became a student again, and it feels wonderful.” 1 month later, April 1968, Dr. Morrison attended his first formal class at Bruce Lee’s school. Wore training clothes, stood in the back with other beginners, practiced basic stance, basic breathing, basic awareness. The chief of orthopedic surgery at Cedars-Sinai Medical Center training alongside college students and construction workers and secretaries, all learning together, all beginners in this tradition.
Bruce taught Morrison personally, patiently, showed him the fundamentals. Breathing technique, stance work, awareness exercises, simple practices that would take months to master, but would provide foundation for everything else. Morrison practiced daily, before work, after work, obsessively, the way he’d practiced medicine, the way he approached everything, with total commitment, total dedication, total focus on mastery.
6 months later, September 1968, Morrison could voluntarily lower his heart rate by 20 beats per minute, could control his breathing to reduce his own stress response, could demonstrate muscle isolation in his core. Not at Bruce’s level. Bruce had decades of practice, but enough to understand the mechanisms, enough to teach basics to others.
Morrison started teaching breathing techniques to his patients. Postoperative pain management, pre-surgical stress reduction, chronic pain control, all documented, all measured, all showing objective benefit. Reduced opioid use, faster recovery times, better patient outcomes. He published a paper in 1969, “Integration of Traditional Eastern Breathing Techniques in Postoperative Pain Management: A Preliminary Study”, co-authored with Bruce Lee.
The first mainstream Western medical journal article to seriously examine Eastern practices through rigorous scientific methodology. It was controversial. Some colleagues dismissed it. Some were intrigued. Some began their own investigations. Morrison brought traditional Chinese medicine practitioners, including Amy Chen’s grandmother, to Cedars-Sinai, not as alternatives to Western doctors, but as collaborators, teaching breathing techniques, teaching acupressure, teaching body awareness, all under Morrison’s supervision, all measured,
all documented. The model worked. Patients benefited. Outcomes improved. Slowly, cautiously, other hospitals began paying attention, began considering that maybe maybe integration was superior to dismissal, maybe Eastern traditions contained practical knowledge Western medicine could learn from. July 20th, 1973, Bruce Lee died in Hong Kong, cerebral edema, age 32.
The news devastated Morrison. He’d known Bruce for 5 years, had studied with him, had learned from him, had collaborated with him on research that was beginning to change how Western medicine viewed Eastern practices. Morrison flew to Seattle for Bruce’s funeral, stood with thousands of others, mourned the teacher who’d shattered his arrogance and replaced it with humility, who’d shown him that real science required openness, not dismissal, that real understanding required integrating multiple perspectives, not defending a single
paradigm. Linda Lee asked Morrison to speak at the funeral, to represent the medical community, to talk about Bruce’s impact beyond martial arts. Morrison stood at the podium, looked at the crowd, at martial artists and actors and students and doctors and people from every background Bruce had touched. “I met Bruce Lee in a hospital room”, Morrison began.
“I was arrogant, dismissive, certain that Western medicine had a monopoly on truth, certain that Eastern practices were pseudoscience. Bruce didn’t argue with me, didn’t try to convince me verbally. He just demonstrated, showed me voluntary control of his heart rate, showed me muscle isolation Western anatomy said was impossible, showed me temperature control Western physiology said couldn’t exist.
And then he helped my patient, taught him pain management better than my morphine had provided. In 15 minutes Bruce destroyed 30 years of my certainty, made me humble, made me a student again. That was 5 years ago. Those 5 years have been the most productive, most enlightening, most transformative of my career. Because Bruce taught me that real knowledge requires integration, that Western and Eastern medicine both have pieces of truth, that being a good doctor means being humble enough to learn from traditions you don’t fully understand.
Bruce changed my practice, changed my teaching, changed how I think about the human body and what it’s capable of. I’m a better doctor because of him. Thousands of my patients have better outcomes because of what he taught me. That’s his legacy, not just the films, not just the martial arts, the lives changed through teaching, through demonstration, through showing people that what they thought was impossible is actually just untrained.
Thank you, Bruce, for your patience, for your teaching, for making me better. I’ll carry what you taught me for the rest of my career, and I’ll teach it to the next generation. Your integration of East and West will continue, will grow, will help people long after you’re gone.” Morrison kept that promise, continued teaching integrated medicine, continued researching Eastern techniques through Western scientific methodology, continued Bruce’s mission of bridging the traditions.
By 1995, Morrison was 79 years old, technically retired but still teaching. The integration Bruce had advocated was becoming mainstream. Acupuncture was offered at major hospitals. Breathing techniques were standard in pain management protocols. Mind-body medicine was recognized as legitimate field. Medical schools were beginning to teach awareness of Eastern practices, beginning to train doctors to be open rather than dismissive.
Morrison taught a course at UCLA Medical School, “Integrated Medicine: Bridging Western Science and Eastern Practice”. It was popular, controversial with older faculty who still believed Western medicine was superior, but popular with students who understood the future of medicine required synthesis, not supremacy.
In his final lecture before retiring completely, Morrison told the story of meeting Bruce Lee, of being arrogant, of being taught humility, of having his certainty shattered by demonstration he couldn’t explain, of learning that the human body was more extraordinary than any single tradition fully comprehended. “Real science”, Morrison told his students, “isn’t defending your beliefs against contradictory evidence.
Real science is changing your beliefs when the evidence demands it. Bruce Lee showed me evidence that contradicted everything I’d been taught. I had a choice, dismiss the evidence to protect my worldview, or change my worldview to accommodate the evidence. I chose change. That choice made me a better doctor, made me a better scientist, made me a better human being.
I’m asking you to make the same choice. When you encounter practices that seem mystical, that contradict what you’ve learned, that come from traditions you don’t understand, don’t dismiss them. Investigate them. Measure them. Test them. See if they work. If they work, learn why. Integrate them. Build better models, better medicine, better understanding.
That’s what Bruce taught me. That’s what I’m teaching you. The human body is more extraordinary than we know. Our job isn’t to defend what we already know. Our job is to discover what we don’t know yet, to integrate, to synthesize, to build something better than either tradition alone. Go forth and be humble. Be curious. Be integrative.
Be better than I was when I met Bruce. Don’t make my mistake of dismissing what you don’t understand. Make my growth of learning what you didn’t know was possible.” Morrison died in 1998 at age 82. His obituary in the Los Angeles Times mentioned his pioneering work in integrative medicine, mentioned his collaboration with Bruce Lee, mentioned the thousands of patients who’d benefited from his willingness to learn from Eastern traditions.
Mentioned the residents and students he’d taught to be open rather than dismissive. Amy Chan, who’d witnessed the original hospital room demonstration, became a licensed acupuncturist. Worked at Cedar-Sinai, the same hospital where Morrison had dismissed Eastern practices, now employed Eastern practitioners, integrated them into patient care, measured outcomes, documented benefits.
Dr. Sara Klein became chief of integrative medicine at UCLA Medical Center. Built programs combining Western and Eastern approaches. Trained the next generation of doctors to understand both traditions. To synthesize rather than choose. Dan Inosanto recovered from his injuries.
Returned to training after 14 months. Walked with slight limp for the rest of his life, but remained mobile, active, teaching martial arts well into his 70s. He taught the breathing technique Bruce had taught him in that hospital room. Taught it to his students. Taught them that martial arts wasn’t just fighting, was body awareness, pain management, voluntary control of functions Western medicine said were automatic.
Taught them integration. The hospital room demonstration on March 8th, 1968, rippled forward. Changed one doctor who changed thousands of patients who changed medical culture, who changed how Western medicine viewed Eastern practices. Changed from dismissal to investigation. From supremacy to integration. From arrogance to humility.
Bruce Lee fought no one that day. Defeated no opponent physically. Just demonstrated. Just showed a skeptical surgeon something that contradicted his certainty. Just proved that the human body was more controllable, more extraordinary, more capable than Western medicine fully acknowledged. In that demonstration, 15 minutes of voluntary heart rate control, muscle isolation, temperature regulation, and pain management changed medical opinion.
Changed careers. Changed lives. Changed how he thousands of doctors approach patient care. Changed the integration of Eastern and Western medicine in America. One afternoon, one hospital room, one demonstration, decades of impact. That’s the power of teaching. Not defeating opponents. Not proving superiority.
Just showing people what’s possible. What they didn’t know they didn’t know. What their certainty prevented them from seeing. Bruce Lee taught a surgeon. The surgeon taught thousands. Those thousands taught millions. The ripples continue. Integration continues. Understanding deepens. Medicine improves.
All because Bruce walked into a hospital room carrying flowers and a book. Met a dismissive doctor and calmly demonstrated that certainty is the enemy of growth. That real knowledge requires humility. That East and West both have truth. That integration is superior to supremacy. The human body is more extraordinary than we know. Our knowledge is always incomplete.
Our frameworks are always provisional. Our certainty is always suspect. Stay humble. Stay curious. Stay open to learning from traditions you don’t understand. That’s what Bruce taught Morrison. That’s what Morrison taught his students. That’s what continues being taught today. One demonstration. Endless teaching. Forever.
Disclaimer : This content may be created by AI for entertainment purposes. Any resemblance to real persons, events, or places is coincidental.